

Abstract
Introduction. The gradient echo multiecho T2* MRI technique is the most robust method for the non invasive, sensitive, and fast quantification of organ-specific iron overload. A crucial aspect is the transferability of the T2* technique among different MRI scanners, in order to expand the availability of high-quality monitoring of iron accumulation to a large population. The intra- and inter-operator reproducibility, inter-study reproducibility, and inter-scanner reproducibility of the T2* MRI method for measuring iron concentrations in the heart and liver have already been demonstrated. However, the transferability of the MRI multislice multiecho T2* technique for pancreatic iron overload assessment has not been evaluated. Thus, the aim of our study was to assess the transferability of this approach among ten MRI sites.
Methods. All subjects underwent MRI using conventional clinical 1.5T scanners of three main vendors. Fifty healthy subjects, five for each site, including the reference centre, were scanned. Five patients with thalassemia were scanned locally at each site and were rescanned at the reference site in Pisa within 1 month.
T2* image analysis was performed using custom-written, previously validated software (HIPPO MIOT®). T2* values over pancreatic head, body and tail were calculated and the global pancreatic T2* value was obtained as the mean. The lowest threshold of normal T2* value was 26 ms6.
Results. On healthy subjects the global pancreas T2* values ranged from 28.93 to 48.89 ms (mean 37.88 ms, SD 5.08 ms). No significant difference was detected among the sites (P=0.334).
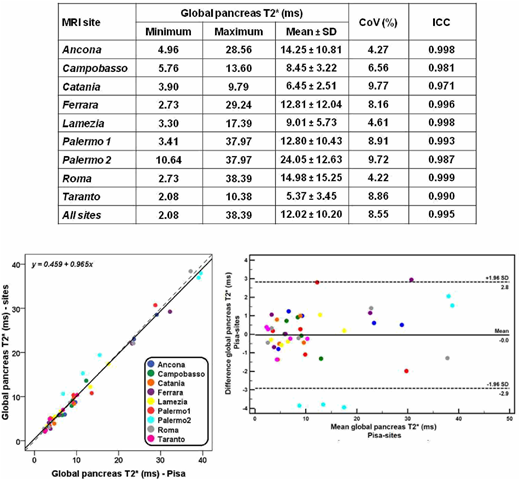
Table 1 shows the global pancreas T2* values measured at the different MRI sites. The global pancreas T2* values ranged from 2.08 to 38.39 ms. There was not a significant difference between the T2* values measured in the MRI sites and the correspondent values observed in Pisa (12.02±10.20 ms vs 11.98±10.47 ms; P=0.808). All patients categorized as having pancreatic iron overload in the MRI sites, fell in the same category after the MRI executed in Pisa.
There was a strong correlation between the global pancreas T2* values calculated from images obtained in Pisa and at the other MRI sites (R=0.978, P<0.0001).
Figure 1 shows the global pancreas T2* values calculated from images obtained at the 9 MRI sites as a function of global pancreas T2* calculated from images obtained in Pisa. The line of best fit had a slope of 0.965 ± 0.021 and an intercept of 0.459 ± 0.328 ms. The R-squared value for the fit was 0.981. Neither constant bias (intercept did not significantly differs from zero) nor proportional bias (angular coefficient did not significantly differ from 1) affected the measurements.
CoVs for all MRI sites are provided in Table 2; they ranged from 4.22 to 9.77%. The CoV for all the T2* values independently from the sites was 8.55%.
The ICC considering all the T2* values, independently from the sites, was 0.995. The ICC for each MRI site is provided in Table 2 and it was always excellent.
The comparison between Pisa and the other MRI sites by Bland-Altman analysis showed a mean absolute difference of -0.04 ± 1.47 ms for the global pancreas T2* values (Figure 2). No bias was present and no greater differences for higher T2* values were detected.
The mean absolute difference in patients with pancreatic iron (N=39) was -0.15 ± 1.38 ms.
Conclusion. The gradient-echo T2* MRI technique is an accurate and reproducible means for the calculation of pancreatic iron and may be transferred between MRI scanners in different centers from different manufacturers.
Pepe:Chiesi Farmaceutici S.p.A., ApoPharma Inc., and Bayer: Other: No profit support.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal